Gastrointestinal and Urinary
Procedure Guide
Obstructive jaundice and/or cholangitis, benign or malignant
Common benign etiologies (10-20%): biliary surgery, liver tx, cholelithiasis, pancreatitis, cholangitis, PSC, cystic fibrosis, cystic disease, radiation
Common malignant etiologies (80-90%): cholangiocarcinoma, pancreatic, gallbladder, HCC, mets
Elevated Alk phos not specific for cholestasis
Often high obstruction (above the cystic duct) as low obstructions can often be treated with endoscopic biliary stent
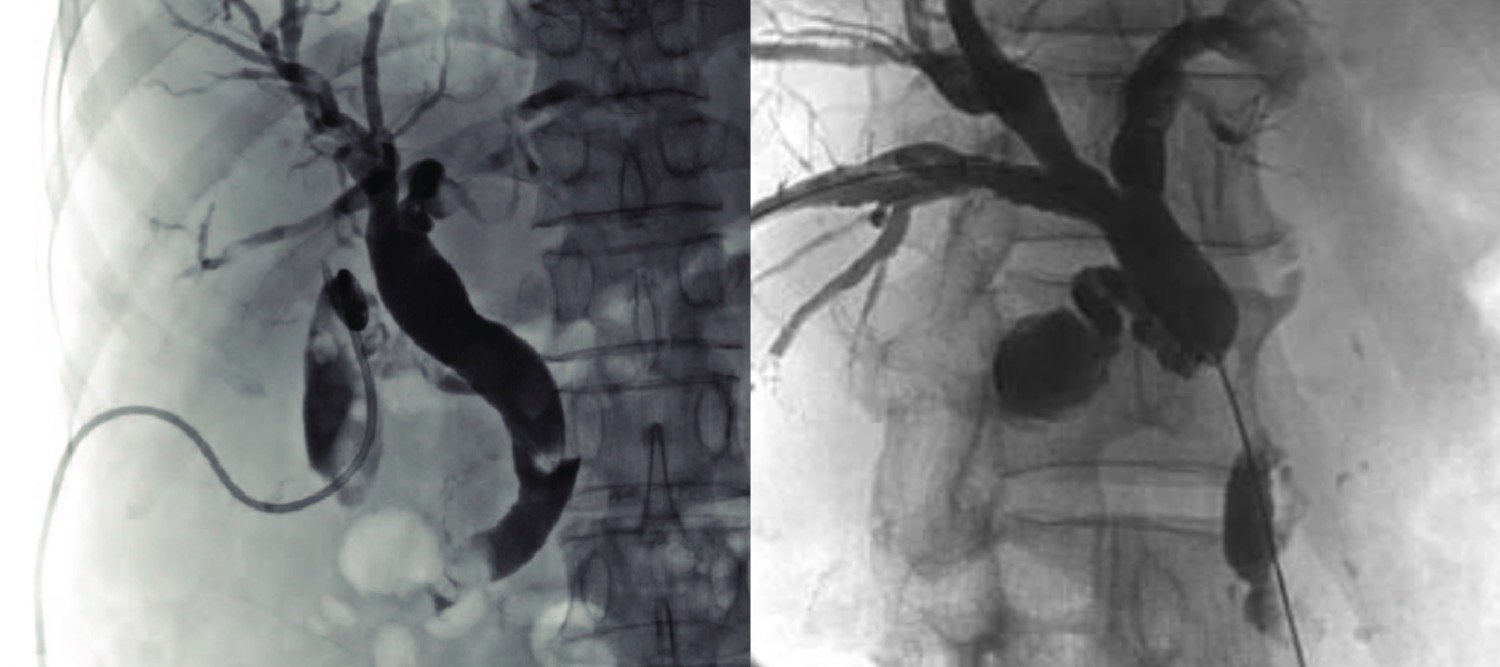
Bismuth and Corlette classification of hilar tumors: (1) hepatic duct w/out hilar involvement; (2) involve hilum (require 2 drains); (3) extension to secondary biliary confluence on right (3a) or left (3b); (4) extensive bilaterally or multiple obstructing lesions
Means of access for biopsy, stent placement, or brachytherapy for cholangiocarcinoma
Biliary diversion for bile leak/biloma
Uncorrected coagulopathy (Plt <50K, INR >1.5)
Asymptomatic segmental isolated intrahepatic obstruction (likely to introduce bacteria and make drain required indefinitely)
Heavy tumor burden with >2-3 isolated obstructions (unlikely to provide benefit)
Polycystic liver disease or echinococcal cysts obscuring safe percutaneous access
PSC and cholecystectomy strictures - won’t help unless cholangitis
(Relative) large-volume ascites, some will do a paracentesis and then place the drain
Endoscopic drain via ERCP: superior for obstruction inferior to liver hilum in term of patient comfort and complications
Percutaneous Transjejunal Biliary Access: better for repeat interventions, non-dilated ducts, multiple bilioenteric anastomosis
Percutaneous Transhepatic Biliary Drain (PTBD): 86-100% technical success; 81-96% successful drainage
Malignant biliary obstruction mortality: 12% @ 30d, 36% @ 3mo, 93% @ 12mo
Negative predictors for clinical benefit: albumin <3.4 g/dL, age >70, Tbili >3.4, poor ECOG, high ASA, persistent hyperbilirubinemia after initial drain placement
Multiple (>1) biliary drains are successful in sufficiently decreasing bilirubin to qualify for additional chemotherapy in ~1 in 3 patients
Stent patency for low CBD obstruction: 95.5% at 3 mo, 92.6% at 6 mo, and 85.7% at 12 mo
US first line to assess for biliary ductal dilation, stone, mass -> MRCP or CT for procedural planning
Often not helpful to drain atrophic segment 2/2 chronic PV thrombus or biliary obstruction
Often not helpful for multifocal strictures (e.g. PSC or diffuse biliary ischemia)
Biliary variants - Huang classification
Huang A1 (65%): R and L bifurcation w/ R bifurcating into Ant and Post
Huang A2 (12%): Ant, Post, L trifurcation
Huang A3 (13%): Post arises from L
Huang A4 (8%): Post arises from common hepatic w/ later Ant and L bifurcation
Huang A5 (2%): Post arises from cystic duct w/ Ant and L bifurcation
Hold coumadin, no need to hold ASA/Plavix
Prophylactic Zosyn at least 1-2 hrs prior to placement. Some patients also need this for exchanges as well. Approximately 25-50% of malignant obstruction biliary systems are infected so transient bacteremia is common during placement.
Consider holding PPI - may increase risk of infection after biliary intervention
Some use general anesthesia or MAC for new placement vs moderate sedation if relatively straightforward
Biliary Drain Placement
Pre-scan and choose duct more peripheral to avoid major blood vessels yet not too peripheral to give a decent transhepatic tract
Area of obstruction often guides access. If right and left thought to be connected, studies suggest left is more comfortable than right.
For non dilated systems, right is often better. More ducts to hit.
Access the biliary tree
Can use needle in access kit or separate 22G IN-RAD, other chiba, 21G thinwall, etc.
Can use ultrasound (left or right) or fluoroscopy (usually only right, high risk with left).
Ultrasound - target longitudinal axis of duct or branch point for greater purchase.
Fluoroscopy (right) - mid-axillary line aiming superiorly towards T12 and slightly anterior centrally and slowly pulling back. Fan inferiorly with each pass.
Challenging /refractory / nondilated tricks
Two stick technique - trying to stick the biliary system centrally under fluoroscopy to opacify the biliary tree and use separate needle to access the biliary tree in a more favorable location.
Aim for peripheral portal vein bifurcation and stick crotch. Pull back slowly as the bile ducts should run nearby.
Contrast injection to confirm access. Only bile duct and lymphatics should flow toward the hilum.
Advance 018 wire, e.g., one in the access kit or Nitrex
Advance access catheter, e.g, Greb set, MAK NV, or Nuff set
Cholangiogram through access catheter (RAO helps lay out ducts)
Cross obstruction if present
If infected, maybe not worth it. If the duct is dissected or perforated trying to cross, time to stop.
Nitrix and curved access catheter from Greb set can be successful. Other can exchange for Kumpe and glidewire. Advancing a sheath can also help for additional support.
Refractory cases: can use TIPS, RF wire, or magnets placed endoscopically and percutaneously
Establish stiff wire access (e.g. amplatz)
Dilate subcutaneous tract
Advance and form biliary catheter. Ideally to have marker not within the parenchyma or jailing off ducts.
Secure catheter in place and apply dressing.
Benign Strictures
Protocols vary - two general approaches are early upsizing to a large drain with cholangioplasty only as needed for initial upsizing vs serial cholangioplasty. Data seems to favor the former, e.g., this RCT suggested repeat cholangioplasty is unnecessary if good result with initial plasty.
Not helpful if fresh anastomosis (<1 month) that may secondary to edema or kink. Better to leave internal-external drain for 2 weeks and then repeat the cholangiogram.
More likely to be successful with shorter, more focal stricture.
End point: resolution of ductal dilation, easy passage of contrast, <20-30% residual stenosis. Transition to capped external drain for 1-2 weeks and then removed if no issues.
Whitaker Test (biliary): External biliary drain is attached to a 3-way stopcock, which is attached to a water manometer and infusion pump to measure the pressure in the biliary tree with infusion.
Place 8.5 or 10.2 Fr internal-external biliary drain -> serial upsizing every 1-2 weeks to 18-20 Fr -> routine exchange every 3 months for 6 months
Primary and secondary patency 81% and 88%, respectively during 20 +/- 12 months of follow up
Place largest internal-external drain tolerated (often 12 or 14 Fr) -> upsize every 2 weeks to a 16-18 Fr silastic drain (Heyer-Schulte) with cholangioplasty only as needed for upsizing -> routine exchange every 3 months for 6-12 months -> 2 week capping trial
1, 2, 5, and 10 year patency of 84, 78, 74, and 67%, respectively
If failed -> surgical revision, biliary stent, or chronic drainage
Duel catheter (“double barrel”) technique:
Cut a 14 Fr internal-external biliary drain ~3-5 cm from the skin
Place 8.5 Fr drain through the 14 Fr drain and out a side hole proximal to the stenosis for effective diameter at stenosis of 22.5 Fr with only a 14 Fr percutaneous access. Has also been done with a balloon catheter through a 14 Fr biliary drain.
One study reported 99% clinical success at 24 months with 9% recurrence at 6-26 months for anastomotic strictures
Endobiliary Biopsy
Brush biopsy not great, yield ~50%
Bile cytology with curved catheter just proximal to malignant obstruction can be diagnostic in 40-60%
Clam shell kits with better tissue, can do with cholangioscopy with yield apparently 95%
Stenting
Plastic stents - generally placed endoscopically but can be placed percutaneously. Require routine exchanges.
Metal stents - generally for malignant strictures with poor prognosis (<1 yr to live)
Issues with long dwell times include clogging and migration. These can be removed percutaneously if necessary.
Classic teaching was that covered stents (e.g. Viabil, Gore) > bare metal stent in terms of patency. However, more recent studies such as this RCT show no difference in patency with bare metal stents more vulnerable to ingrowth and covered stents more vulnerable to clogging from sludge. ~50% occlusion in 10 months.
Ideal to avoid covering the cystic duct or coursing through the sphincter of Oddi if possible.
Potential longer patency and better survival with endobiliary RFA (e.g. Habib, Boston Scientific) or external beam radiation applied to obstructing lesion. See this RCT and meta-analysis.
Activated for 90 sec followed by resting/cooling for 60 sec. Post ablation balloon sweep with balloon, e.g., Fogarty to clear debris
Options for central/hilar obstructions
Stent across right to left with uncovered stent and balloon out the side into the CBD with additional stent in a T-configuration
Kissing stents into the right and left into a CBD stent in a Y-configuration
Uncovered stent from the right or left into the CBD and then balloon out the side into the contralateral side with additional stent in a Y-configuration
Choledocholithiasis
Ideal to sweep stones into duodenum rather than out percutaneous access with Fogarty to Python balloon catheter. However, stones >6 mm require pre-sweep plasty of the ampulla and stone >15 mm require lithotripsy.
Drain Placement:
Early:
<1% death
5-10% major complications: sepsis (2.5%), hemorrhage (2.5%), inflammatory/infectious (1.2%, abscess, peritonitis, cholecystitis, pancreatitis), pleural fistula (0.5%)
66% minor complications: hemobilia, fever, transient bacteremia. Other studies report lower rates.
Late: cholangitis, catheter dislodgement, peritonitis, hypersecretion of bile, cholecystitis, biliopleural fistula, skin infection, intra/parahepatic abscess, metastatic seeding
Endobiliary Ablation vs Stenting Alone: increased risk of post-procedural abdominal pain (21% vs 10%), bleeding (12% vs 4%), and bile leak (0.6% vs 0.3%). Similar rates of cholangitis (~6-7%) and pancreatitis (3-4%).
Hospitalization & monitoring at least 24 hrs. Some suggest continued antibiotic coverage.
Flush drains with 10cc saline 1-2xs per day. Drain should be exchanged every 2-3 months.
External drainage can cause dehydration. Patients should hydrate aggressively
Monitor bilirubin - should drop 50% in 10-15d. Interval increase should prompt drain check.
Pericatheter leakage - often secondly to kink, occlusion, or displacement. -> drain check with upsizing as last resort
Sepsis -> assess for occlusion or undrained ducts, if external catheter is capped try uncapping to allow external drainage
Hemorrhage -
Venous - often secondary to side hole positioning and will resolve on own; hemobilia alone w/out peri-drain bleeding; hours to days after placement -> sheath study
Arterial- often secondary to drain erosion days to weeks after placement; hemobilia AND peridrain hemorrhage -> angiogram